Looks like New Zealand got rid of it:
https://www.cbsnews.com/news/new-zealand-declares-end-coronavirus-prime-minister-jacinda-ardern/
BTW, how did Switzerland's strategy turn out?
They had 16 new cases yesterday. Nationwide.
Looks like New Zealand got rid of it:
https://www.cbsnews.com/news/new-zealand-declares-end-coronavirus-prime-minister-jacinda-ardern/
BTW, how did Switzerland's strategy turn out?
Did they stick with keeping things open, shooting for herd immunity and isolating the vulnerable? Or did they do a course correction somewhere along the way?They had 16 new cases yesterday. Nationwide.
They partially shutdown, implemented massive testing and tracing, blocked pretty much everyone from entering the country back in February I believe.Did they stick with keeping things open, shooting for herd immunity and isolating the vulnerable? Or did they do a course correction somewhere along the way?
Did they stick with keeping things open, shooting for herd immunity and isolating the vulnerable? Or did they do a course correction somewhere along the way?
Switzerland didn't keep things open, they locked down. You're probably thinking of Sweden who kept things open. Their per capita death rate is now higher than the US. The guy who designed their response has admitted he thinks they should have done more.Did they stick with keeping things open, shooting for herd immunity and isolating the vulnerable? Or did they do a course correction somewhere along the way?
The reason I asked is because I had this post in mind:Switzerland didn't keep things open, they locked down. You're probably thinking of Sweden who kept things open. Their per capita death rate is now higher than the US. The guy who designed their response has admitted he thinks they should have done more.
Note: This following info is from a poster in Switzerland. So cannot verify the veracity, but does match the little press I have seen.
Switzerland is also taking a different approach. They are not shutting down, but isolating the vulnerable population (over 60, health concerns...). Schools stayed open, when closing, they are offering child care so grandparents do not watch the kids, restaurants, gatherings all continuing. Elderly expected to stay away, join family virtually... The idea is the health system has the capacity to handle the cases based on the lower rate you get with the younger population. This will then basically generate herd based immunity, and make it more manageable when it eventually gets to the vulnerable.
Roger that. That post was from 3/15. From what I can find online, they imposed additional lockdown measures after that date.The reason I asked is because I had this post in mind:
https://www.pilotsofamerica.com/com...-the-silver-lining.124889/page-3#post-2889261
Since it is common knowledge I'd say yes. You'll find Google very helpful in this regard.
Where can I get me some?SARS antibodies block coronavirus infections, study shows
https://www.sfchronicle.com/bayarea...ies-block-coronavirus-infections-15331566.php
Abstract
"SARS-CoV-2 is a newly emerged coronavirus responsible for the current COVID-19 pandemic that has resulted in more than 3.7 million infections and 260,000 deaths as of 6 May 20201,2. Vaccine and therapeutic discovery efforts are paramount to curb the pandemic spread of this zoonotic virus. The SARS-CoV-2 spike (S) glycoprotein promotes entry into host cells and is the main target of neutralizing antibodies. Here we describe multiple monoclonal antibodies targeting SARS-CoV-2 S identified from memory B cells of an individual who was infected with SARS-CoV in 2003. One antibody, named S309, potently neutralizes SARS-CoV-2 and SARS-CoV pseudoviruses as well as authentic SARS-CoV-2 by engaging the S receptor-binding domain. Using cryo-electron microscopy and binding assays, we show that S309 recognizes a glycan-containing epitope that is conserved within the sarbecovirus subgenus, without competing with receptor attachment. Antibody cocktails including S309 along with other antibodies identified here further enhanced SARS-CoV-2 neutralization and may limit the emergence of neutralization-escape mutants. These results pave the way for using S309- and S309-containing antibody cocktails for prophylaxis in individuals at high risk of exposure or as a post-exposure therapy to limit or treat severe disease."
The paper:
https://www.nature.com/articles/s41586-020-2349-y_reference.pdf
"This is a PDF file of a peer-reviewed paper that has been accepted for publication. Although unedited, the content has been subjected to preliminary formatting."
I posted these links in a thread that is now closed. I was hoping that someone knowledgeable could comment on the methodology and/or conclusions:
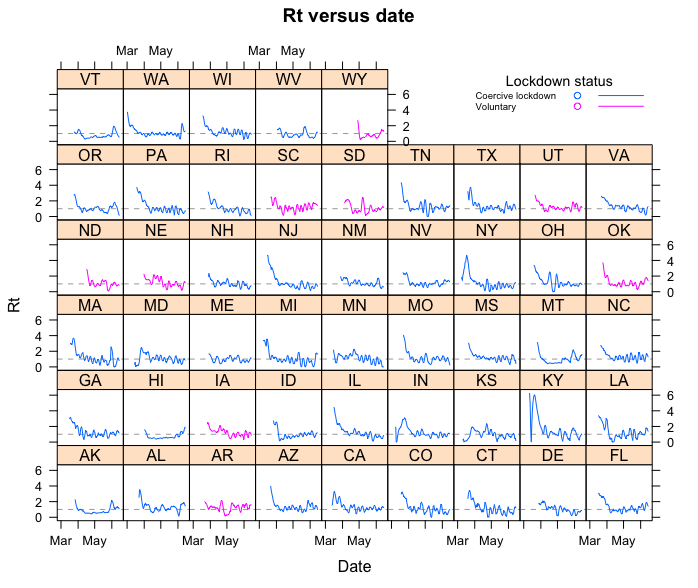
Differential Effects of Intervention Timing on COVID-19 Spread in the United States
https://www.medrxiv.org/content/10.1101/2020.05.15.20103655v1.full.pdf
Out of curiosity, what exactly are you reading to get that?My read right now is that warmer weather is tamping this down, like it does with the common cold.
The reason for 3 weeks, is, sequestered in the house, one of transmission is covered....(roughly, 11 days x 2)
Out of curiosity, what exactly are you reading to get that?
Certainly hasn’t been true for vast majority of southern states. Arizona is skyrocketing and temps have been around 110F.
Out of curiosity, what exactly are you reading to get that?
While that appears to be true for Georgia, many of the warmer states appear to be making significant new highs in numbers of new cases.a post from 3-4 weeks ago? Not a clue what I was specifically looking at. I suspect I was watching the graphs. In mid May, the numbers for Georgia were trending downward despite the state opening up. So businesses were opening and people were and are getting out, but the numbers weren’t really going up. May was about 10-15 degrees warmer, so it seems like a reasonable hypothesis.
Even now, despite so many people being out, the numbers are not even close to the highest numbers.
While that appears to be true for Georgia, many of the warmer states appear to be making significant new highs in numbers of new cases.
https://www.nytimes.com/interactive/2020/us/coronavirus-us-cases.html#states
(Scroll down about 1/6 of the way from the top.)
first, the data is very noisy.
second, increases in reported cases could be caused by increases in the number of test performed. When have the various States reached a point when there was no shortage of testing capacity available?
Bob,
Most of the states showing increases in cases are also getting increases in positivity rate. I do not follow the math well enough to explain it; but assuming I understand it the concepts:
1. If the case counts are increase just due to expanded testing the test positivity rate should be decreasing as you find it harder to find positive cases.
2. Higher positivity rates actually mean that the virus is actually spreading more unchecked and we have less of a handle on the actual cases, and are more likely to be under reporting cases.
Note: I did not check, but another poster posted charts for AZ which makes the situation in AZ look so bad. Case positivity rate, testing rates and case counts are all increasing. But not equally, the positivity rate went from roughly 7% to 40% based over a four week period. Per the poster, this means the number of cases is rapidly increasing.
Tim
I wasn't expressing an opinion on whether people should continue to be confined. I just think that's it's important to know what the data really are, however imperfect they may be.Yes, although some of these states, such as Arizona, didn’t ever really have a high to begin with. It’s likely the current spikes are due to people vacationing during Memorial Day as well as quarantine exhaustion.
You cannot confine healthy people indefinitely. Until this year “quarantine” always meant sick people for a reason.
If you need the CDC to tell you basic things about influenza you should really get out more. That is, after the present imbroglio relents.I wonder when the CDC will google to find your common knowledge.
1. What I meant by increased testing causing an increase includes consideration of the scenario of testing not being complete enough. Until there is a surplus of testing capacity, rationing testing will (possibly) miss a number of positive cases. Once there is sufficient testing capacity to test everyone that is showing symptoms and everyone who has been even minimally exposed to someone symptomatic (or positive), then testing beyond that would likely only being testing people who would be negative (unless there are a lot of asymtomatic people).
2. Sure, if the virus is spreading, then you would generally expect more positive results. However, increases in positive rates could simply be the result of better focused testing.
https://www.azdhs.gov/preparedness/...se-epidemiology/covid-19/dashboards/index.php
doesn't seem to indicate a positive rate going from 7% to 40%. The positive rate is noisy week to week. And isn't much higher than the positive rates of some weeks in April.
It looks like Arizona didn't really ramp up testing until May.
Bob,
Most of the states showing increases in cases are also getting increases in positivity rate. I do not follow the math well enough to explain it; but assuming I understand it the concepts:
1. If the case counts are increase just due to expanded testing the test positivity rate should be decreasing as you find it harder to find positive cases.
2. Higher positivity rates actually mean that the virus is actually spreading more unchecked and we have less of a handle on the actual cases, and are more likely to be under reporting cases.
Note: I did not check, but another poster posted charts for AZ which makes the situation in AZ look so bad. Case positivity rate, testing rates and case counts are all increasing. But not equally, the positivity rate went from roughly 7% to 40% based over a four week period. Per the poster, this means the number of cases is rapidly increasing.
Tim
I wasn't expressing an opinion on whether people should continue to be confined. I just think that's it's important to know what the data really are, however imperfect they may be.
1. What I meant by increased testing causing an increase includes consideration of the scenario of testing not being complete enough. Until there is a surplus of testing capacity, rationing testing will (possibly) miss a number of positive cases. Once there is sufficient testing capacity to test everyone that is showing symptoms and everyone who has been even minimally exposed to someone symptomatic (or positive), then testing beyond that would likely only being testing people who would be negative (unless there are a lot of asymtomatic people).
I would like to know that too, but I'm resigned to the fact that it's unanswerable for now. It not only has to do with local or national (ours) regulations, but also regulations in places you might like to roam in the world. Of course there is sneaking outThat is all well and good but I would still like to know when we might be able to roam freely on the earth, so to say.
") , but that's much easier within the country than outside of it.
, but that's much easier within the country than outside of it.Me too!That is all well and good but I would still like to know when we might be able to roam freely on the earth, so to say.
I've been mostly staying home, but I've been skipping the cowering part. Am I in trouble?Count me as someone else who won't cower in my home.