Pinecone
En-Route
I saw some info that the 2024 FAA Reauthorization Act may include changes to BasicMed, loosening the restrictions.
Supposedly
1) Increases passengers allowed to 6
2) Increases seats allowed to 7
3) Increases max certificated takeoff weight to increase to 12,500 pounds.
4) Would require FAA to help work on getting it accepted in other countries
5) Allow DPEs to do administer tests or proficiency tests with Basic Med
If this is true, I suggest two things.
1) Contact your Congress members (Senate and House) to support this.
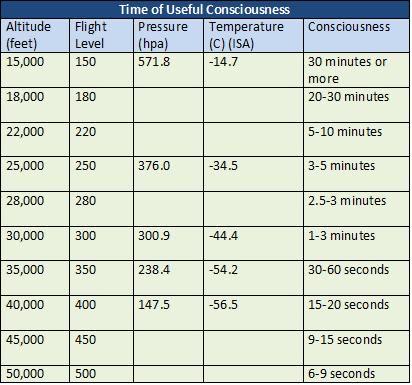
AND, add on my change, allow Basic Med up to at least FL250.
To contact your Congressional reps, go to - https://www.congress.gov/
This website will give you the info on your representatives by your address. For each one, there is a Contact link, which takes you to their website, where you can enter your info and your request.
This is what I sent to my representatives:
I understand that the 2024 FAA Reauthorization Act contains some changes in the limitations when acting as a pilot under the Basic Med provisions.
I would like to request that you support these changes. The FAA recently published a study that shows no difference in the mishap rate for people on Basic Med versus the traditional medical certification.
I would also like you to introduce and support one other change to the limitations for Basic Med and that is to increase the allowable maximum operating altitude from the present 18,000 feet to a minimum of Flight Level 250 (25,000 feet). Flight Level 280 would be even better.
I do want to applaud Congress for mandating the Basic Med program and making that happen. It makes sense to deal with my primary care physician, who knows me well versus a doctor who sees me for 30 minutes every two years.
Thank you.
Supposedly
1) Increases passengers allowed to 6
2) Increases seats allowed to 7
3) Increases max certificated takeoff weight to increase to 12,500 pounds.
4) Would require FAA to help work on getting it accepted in other countries
5) Allow DPEs to do administer tests or proficiency tests with Basic Med
If this is true, I suggest two things.
1) Contact your Congress members (Senate and House) to support this.
AND, add on my change, allow Basic Med up to at least FL250.
To contact your Congressional reps, go to - https://www.congress.gov/
This website will give you the info on your representatives by your address. For each one, there is a Contact link, which takes you to their website, where you can enter your info and your request.
This is what I sent to my representatives:
I understand that the 2024 FAA Reauthorization Act contains some changes in the limitations when acting as a pilot under the Basic Med provisions.
I would like to request that you support these changes. The FAA recently published a study that shows no difference in the mishap rate for people on Basic Med versus the traditional medical certification.
I would also like you to introduce and support one other change to the limitations for Basic Med and that is to increase the allowable maximum operating altitude from the present 18,000 feet to a minimum of Flight Level 250 (25,000 feet). Flight Level 280 would be even better.
I do want to applaud Congress for mandating the Basic Med program and making that happen. It makes sense to deal with my primary care physician, who knows me well versus a doctor who sees me for 30 minutes every two years.
Thank you.
")