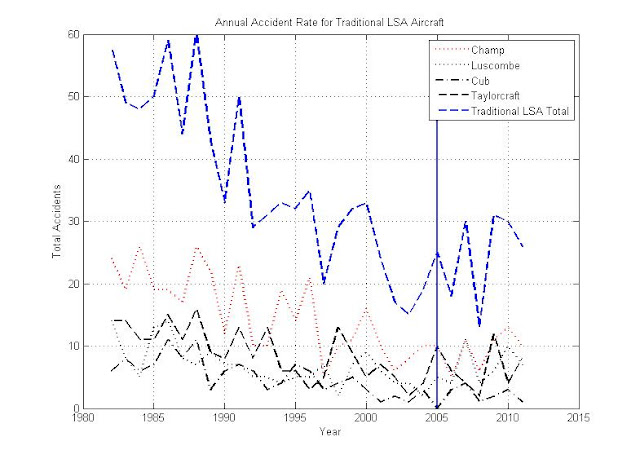
That's accidents per year, not accidents per 100,000 hours flown. The LSA accident rate is really quite a bit taller than the rest of aviation.....per hour. Say whatever you wish to forward you cause but recognize that it doesn't make it true.
1) What does the fact that people wreck little lightly loaded aircraft more than larger, more stable, aircraft have to do with medicals? You have to look at the same population of aircraft with and without the medical requirement to factor out the airplane size effect. The data I plotted was for the same population of aircraft before and after the sport pilot rule.
2) Nobody really knows how many hours these aircraft are flown. And, no one really knows how many Private and "better" pilots are now flying under the sport pilot rules. How do you determine how many hours these aircraft are flown?
3) Unless people suddenly stopped flying these aircraft when the requirement for a medical went away, then the accident rate per 1000 hours did not go up.
Say whatever you want, but this is the only apples to apples comparison you can make. Looking at the accident rate for aircraft that didn't exist before the LSA rules tells you nothing WRT the effect of the medical and not that former Bo drivers wreck light airplanes.
Other factors i n these numbers are economic - how much do people fly. Also you can see shifts between different types of aircraft. If you look at the Cessna 172 vs. the Cessna 150/152 you can see the shift from the 150/152 to the 172 in popularity.The accidents in 172's did not decline with the 150/152 as the economy tanked. You should see a similar thing with implementation of the sport pilot rules as a lot of people have come out of the woodwork and started flying again (like myself). It would be reasonable to expect the accident rate per year to go UP for the "traditional LSAs" as they get pulled out of the corners of hangars and put back in the air (this trend is also reflected in the prices of similar LSA vs. not LSA aircraft).
So, there is every reason to expect that for a given LSA, the number of accidents per year would increase just because of improvements in the economy and the increase in hours per aircraft flown as the geezers get back in the game. And, since we really don't see any statistically significant increase even with those factors, it's really hard to claim that the lack of a medical has any statistical significance in the accident rate for these aircraft no matter how you measure it.
Are pilots flying under the sport pilot rules having medical issues and even accidents related to those issues? No doubt. But so are airmen with valid medicals.
Is the LACK OF A MEDICAL resulting in a significant increase in the number of accidents in the
same population of aircraft? If so, it can't be seen in the data.
Trying to guess how many hours these aircraft are flown isn't going to change the results unless you try to claim that before the sport pilot rules they were flown X hours per year and after they are flown X/2 hours per year - which would be contrary to any reasonable analysis.

 the problem is more with entrenched bureaucrats protecting and expanding their fiefdoms....
the problem is more with entrenched bureaucrats protecting and expanding their fiefdoms....

