PeterNSteinmetz
En-Route
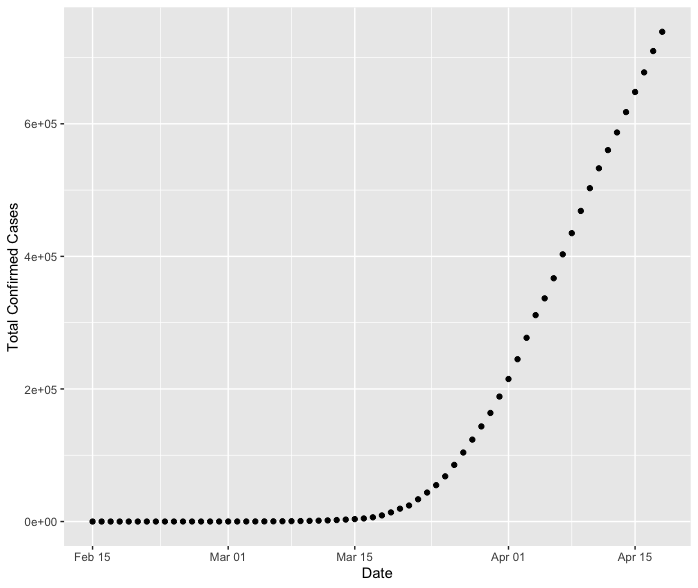
Both the US overall or NY state data has not grown linearly. You can see that by simply examining a full plot of the raw data. It's not a straight line. Both caseload and deaths data has closely followed a canonical logistic curve, which is a self-limiting exponential growth function typical of phenomena like epidemics.
No of course the confirmed cases are not a straight line overall. The question is, if you look at this on a log scale, once there were a reasonable number of cases it appeared to be on an exponential growth curve. Then for the last 4 weeks it has looked quite linear. See attached.
When I attempt to fit the total number of cases with a 5 parameter log-logistic model in R the fit for the same datapoints looks like the following (sorry about the sloppy scale labelling):
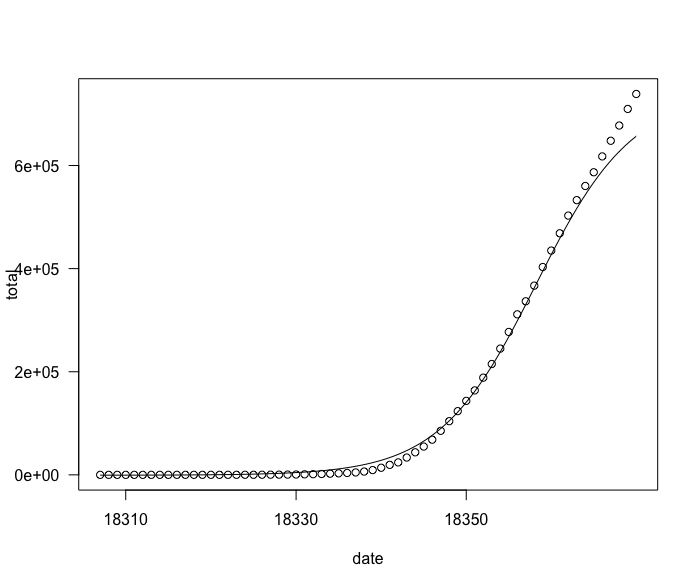
So I am wondering how one distinguishes a case where there is some underlying linear growth factor which has taken over from the case of a log-logistic model with a higher maximum so the curve doesn't turn over like that yet? I guess there is likely a way to make such a model comparison in R, but practically, at this point would one be able to distinguish those two alternatives in a statistically significant manner? It seems like the data may just not really be able to distinguish this but the normal course of epidemics would suggest there is a higher limit involved here where it will turn over. I guess I have to go read the IHME model...
